The acromioclavicular joint (ACJ) is the articulation between the collarbone and acromion. It is located at the tip of the shoulder and stabilized by the capsule and coraco-clavicular ligaments (CCL).
Arthritis:
Trauma or age related ‘wear and tear’ can cause degeneration and loss of cartilage.
The joint literally wears out, develops extra bone (spurs and osteophytes). First line of treatment options are physiotherapy and anti-inflammatory medication. Cortisone injections can also be considered and will provide a temporary solution. Failure of conservative treatment and ongoing symptoms may require surgery and removal of the ACJ is a successful operation which has been described by Mumford in 1941. This operation can be done either keyhole (arthroscopically) or as an open procedure.
Dislocation:
A direct blow to the shoulder or a fall can result in a dislocation of the ACJ with the collarbone displacing upwards, posterior or anterior and inferior. 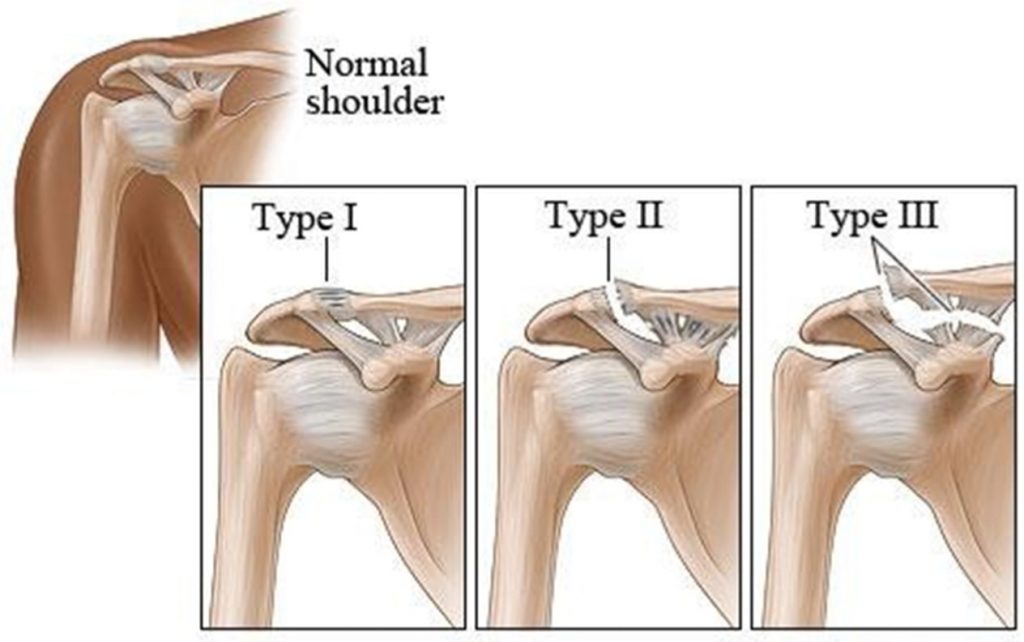
If the capsule is sprained or disrupted (Grade 1 or 2), the joint is considered stable and a sling for comfort is appropriate. If the coraco-clavicular ligaments(CCL) are disrupted surgery should be considered. With acute injuries arthroscopic assisted fixation is a good option. The typical cut-off is at around 3 weeks. With chronic injuries reconstruction of the CCL is required.
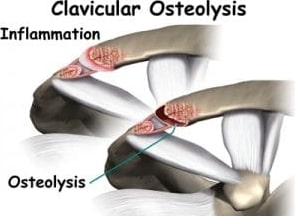
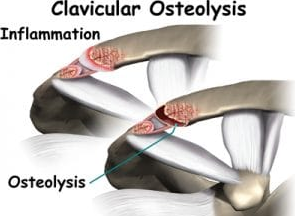
Osteolysis:
Osteolysis or bone erosion is an uncommon condition and occurs commonly in weightlifting athletes who perform repetitive overhead activities and with heavy manual work.